
In no way does this chapter encourage anyone to use medication without the guidance of a specialist; it is only meant to clarify that even couples with infertility issues can, indeed, get pregnant. So let’s get started!
Many women may have issues such as PCOS (Polycystic Ovary Syndrome). This syndrome can interfere with getting pregnant because the ovaries are compromised with several eggs that didn’t leave their “home.” Let’s say they didn’t get the final push, like a cake that didn’t rise because it lacked baking powder. Normally, after growing, eggs receive the LH hormone which makes them, the eggs, leave the follicle and be available for fertilization. Since this doesn’t happen, what should you do in such cases when you want to get pregnant? Treat it!
There are medications that help clear microcysts from the ovaries. The traditional options are Metformin or Glifage for diabetics to help lower blood sugar, or even appropriate birth control pills like Selene and Diane 35, which are quite effective. However, these are contraceptives and will prevent pregnancy. This procedure is also valid for women without PCOS who only have microcysts once in their life.
Another medication that can be very useful for women with polycystic ovaries is Cicloprimogyna. It regulates hormones while not preventing the woman from becoming pregnant. We should remember that every body is unique and may react differently to each medication. That’s why I stress that it’s best to seek a doctor willing to help you in the best way possible and continue treatment until the end, until the ovaries are clear.
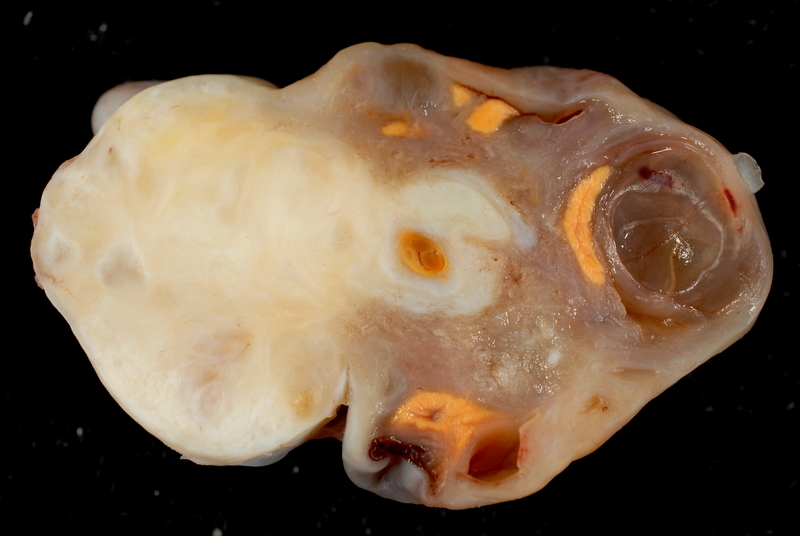
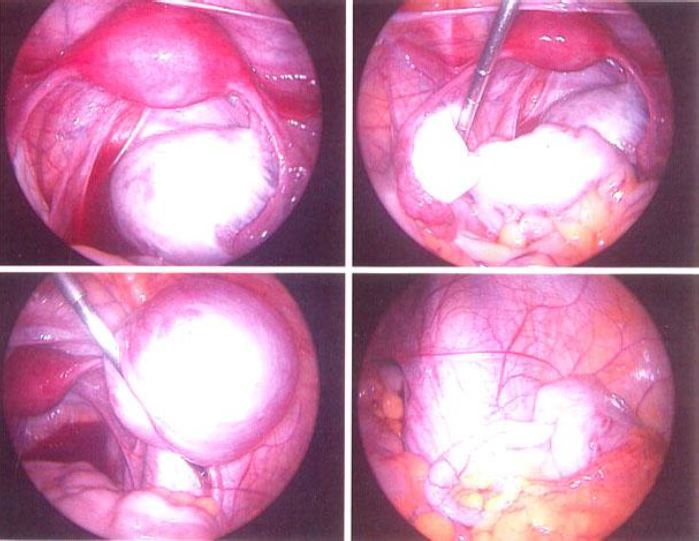
Another infertility disease that affects many women is endometriosis. Unfortunately, it is more serious than PCOS and may permanently prevent pregnancy, not to mention the intense pain. Endometriosis is menstrual blood that leaves the uterine cavity and “sticks” to the inner and outer walls of the uterus, the ovaries, the abdomen, and can even reach beyond these areas, to the intestines or the bladder. How much it affects fertility depends on the severity of the disease. In some cases, only fertility treatments like in vitro fertilization can resolve the situation. Women with endometriosis are—in my opinion—the ones who suffer most from not knowing for sure what can happen, as well as the tremendous pain the disease brings. Even with treatments such as laparoscopy to remove the blood, living with endometriosis is very painful.
Thrombophilia is a disease that does not prevent a woman from getting pregnant, but can cause recurrent miscarriages. Essentially, it is a tendency for blood to clot in the arteries and veins of the woman’s body, including during pregnancy. Imagine a blood clot in the umbilical cord or in the vein that carries oxygen to the placenta and baby! This greatly affects pregnancy and can lead to miscarriage. Women who have had consecutive miscarriages should seek more detailed investigation with their doctor regarding the factors that led to them, including analysis of proteins C and S, whose absence in the body may be linked to thrombophilia. The treatment is simple. For non-pregnant women, anticoagulants such as injectable Heparin and oral low-dose Aspirin should be used. For those already pregnant, injectable or subcutaneous Heparin may be used to thin the blood.
Another rarely discussed problem is tubal blockage. Generally caused by some infection or a sexually transmitted disease such as chlamydia or syphilis, adhesions—as they are called—can interfere with a woman’s ability to get pregnant by preventing the egg from passing through the tubes to be fertilized. This is a possibility that the doctor must consider when investigating female infertility. There is a test, with a name that sounds like a curse word or a German term—hysterosalpingography—that can be done to detect the problem. It is simply an X-ray with intrauterine contrast. It’s quick, easy, and almost painless. I did it some time ago and don’t consider it a big deal; suffering because you can’t get pregnant is much worse.
Treatment for this problem is usually done during the exam itself. If adhesion or blockage of the tubes is found, it can be separated and the tube cleared right then and there. They say that the cycle in which the procedure is carried out is also the best for getting pregnant. Stay strong and go for the hystero if your doctor orders it—no need to be afraid!
Table of Most Common Problems
| Problem | Who | Frequency* | Diagnosis | Treatment |
| PCOS | Woman | 1:5 | Imaging Exam, Blood Test | Hormonal with Birth Control, Metformin |
| Endometriosis | Woman | 1:10 | CA125 Blood Test, Imaging Exam | Medication, Surgical** |
| Thrombophilia | Woman | 1:10,000 | Blood Test | Medication |
| Tubal Blockage | Woman | 1:10 | Hysterosalpingography | Surgical |
| Tubal Adhesion | Woman | 1:8 | Hysterosalpingography | Surgical |
| Sperm Allergy | Woman | 1:30 | Post-Coital Test | Insemination |
| Hostile Mucus | Woman | 1:50 | Post-Coital Test | Insemination |
| Testicular Infection | Man | 1:10 | Semen Analysis, Blood Test | Antibiotics |
| Varicocele | Man | 1:5 | Ultrasound | Medication, Surgical** |
*Estimated frequencies from experience
**If medications are unsuccessful
A lesser-known problem is sperm allergy to the husband. Have you ever heard of this? I imagine not because it is very unusual. This is when your body attacks and destroys sperm, or even prevents it from reaching the uterus for fertilization, creating a hostile, unfriendly environment. Treatment in this case is more complicated, as it may require a financial effort from the couple to pay for the procedure, which unfortunately is not covered by the public health system or most insurance: fertilization or artificial insemination after sperm washing to eliminate the irritant factor in the woman. This usually works very well, but by the time the allergy is diagnosed, a lot of time may have been lost and many tears shed without knowing why pregnancy wasn’t possible. That’s why it is very important to bring this possibility up with your doctor so it can be investigated as a cause.
It’s not just women who can have problems—sometimes they come from the man. Many men still resist admitting the possibility of having any problem that could prevent pregnancy, but it’s worth reminding them of this possibility. Even if he’s already had children, testicular infection at another time could now compromise his fertility. Therefore, checking sperm health is highly advisable. The solution is a semen analysis. If low motility or an anatomical alteration is detected, it becomes easier to treat the real cause of infertility. Usually, these issues are treated with vitamin E and antioxidants. Vitergan is also frequently used. Men are advised to change both their eating habits and even their underwear (tight briefs suffocate the swimmers). Let’s set them free so they can reproduce easily, freely and without obstacles!
To check if everything is ok with your husband’s sperm or your own cervical mucus, why not suggest a post-coital test to your doctor? This is simply an analysis of cervical mucus from the vagina six hours after intercourse. It will show how the ejaculated sperm are doing inside the female cavity and determine if the environment is favorable for them to reach the egg. Remember, this test should always be used alongside semen analysis.
If everything has been investigated and no problems are found but there’s still no pregnancy, it’s time to relax, forget about it, let time pass, or look for a specialist to help with procedures such as timed intercourse, which make it easier for couples with unexplained infertility to conceive.




