
Let’s better understand the female menstrual cycle, because everything starts with the first period. The menstrual cycle exists to show that a woman is now capable of having children. So, from puberty, which starts with the first menstruation for girls and with the first ejaculation for boys, getting pregnant is possible. Menstruation initially occurs with the stimulation of hormones; that is, a woman becomes able to conceive from the moment all the necessary hormones are activated.
Progesterone, estrogen, FSH and LH are responsible for the entire female ovulatory cycle. First, FSH (follicle stimulating hormone) comes into play, produced by the pituitary gland in the brain and, as its name suggests, stimulates the ovarian follicles (the woman’s seed) to grow and mature, so that the woman will ovulate. After about a week of stimulation, FSH stops being produced and only the largest, dominant follicles continue. Sometimes, up to 30 eggs can be stimulated by FSH, and only one becomes viable to be released, mature enough to be fertilized and thus enable pregnancy itself.
From the day when FSH hormone stops being produced, estradiol or estrogen begins to dominate, causing the endometrium (inner lining of the uterus) to thicken, which creates a soft bed for the future baby. The estradiol hormone also finishes growing and maturing the eggs, allowing the LH hormone to take action. This then leads to actual ovulation, releasing the egg from the follicle where it grew. That egg leaves its cocoon and is carried into the fallopian tube, where it waits quietly for up to 24 hours for contact with a sperm to create a baby and, with fertilization, bring about one more miracle of life!
That’s why a woman should have sexual intercourse during her fertile period, because only then is the egg available for fertilization. To determine the right days, you need to know your body a little and recognize the signs of ovulation. The main ones are:
- The Mucus
- The Annoying Cramps
… and some tricks that we will see later on.

After ovulation, another hormone rises in the woman’s body and will be responsible for maintaining the pregnancy to the end, in case she gets pregnant: progesterone. This hormone, when high and in excess, is responsible for the absence of menstruation. That’s why a pregnant woman does not menstruate! Too technical? Put simply, one hormone leads to another, and all of them are essential for a woman to get pregnant. If just one is out of balance, pregnancy may not happen.
Seeking a second pregnancy, I started to learn about my body and recognize its signs, something every woman trying to conceive should do. You should observe these details by asking yourself the following three questions:
- How many days is my cycle?
- Do I have a regular cycle?
- What is my period like?
With these answers, you can detect what type of ‘trying to conceive’ woman you are. Among the types, I usually use these terms:
Punctual: Like clockwork! Every cycle comes on the same day and, in some cases, even at the same time.
Irregular: Every cycle is 2 or 3 days late, but even so, it’s a regulated irregularity.
Roller Coaster: Completely out of control, the period comes on different days in each cycle and it’s never possible to accurately predict when it will show up.
Unexpected Events: Needs medical supervision to be able to get pregnant.
How to Calculate the Fertile Window?
First of all, we must consider that a woman needs to have an active sex life to conceive or, simply, be lucky enough to have intercourse on the exact day of ovulation. But then, how can we detect the most fertile days for each trying-to-conceive woman?
For punctual types, calculating the fertile period is the simplest. Its typical duration is seven days, and the most fertile day is the 14th day before the next period. The three days before and after the most fertile day complete the fertile week. So it’s a simple calculation to determine your fertile days, for example:
Most Fertile Day
28-day cycle: 28 – 14 = 14, that is, the most fertile day is the 14th day of the cycle.
32-day cycle: 32 – 14 = 18, so your most fertile day is the 18th day of the cycle.
Start of Fertile Week
28-day cycle: 28 – 14 – 3 = 11, that is, starts on the 11th day of the cycle.
32-day cycle: 32 – 14 – 3 = 15, so it starts on the 15th day of the cycle.
End of Fertile Week
28-day cycle: 28 – 14 + 3 = 17, that is, ends on the 17th day of the cycle.
32-day cycle: 32 – 14 + 3 = 21, so it ends on the 21st day of the cycle.
The problems start with those trying with irregular cycles. They tend to take longer to conceive precisely because their fertile days are scattered. Unless you and your husband have the willpower to try for more than 30 days straight with daily intercourse (whew!) or happen to hit the exact ovulation day, getting pregnant can be an issue. The same goes for the roller coaster type, who may find it even harder since they don’t know when their fertile window will be.
For those with polycystic ovary syndrome or simply polycystic ovaries (the unexpected events type), treating the condition before starting to try is essential. The disease can disrupt ovulation, causing eggs not to mature properly and to be released for no reason. That’s why women with polycystic ovaries need to clear their ovaries before trying. All of this, of course, without rushing! But realistically, this is a bit impossible for anxious women like I was.
Detection Methods
I myself was the roller coaster type for a large part of my trying-to-conceive journey. But with knowledge of the methods for getting pregnant, I ended up detecting ovulation in cycles of 70 days, and other times I was more irregular with cycles of 30, 32, or 36 days. So, what did I learn during this time trying to conceive? Ways to figure out when I ovulated. The methods I used were the most basic:
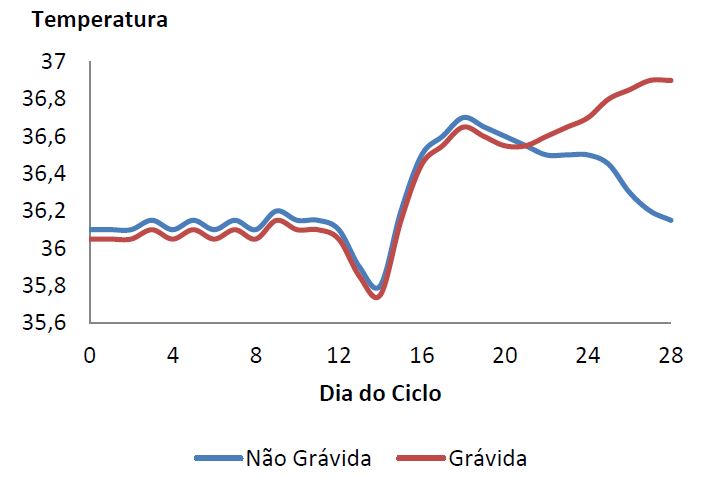
Basal Body Temperature Method: This involves measuring your temperature first thing in the morning, strictly, with a thermometer in hand, moving as little as possible after waking from at least six hours of sleep. Ovulation is detected by a pattern on the temperature chart, where a significant drop followed by a noticeable rise may indicate ovulation – and all that happens because of hormones! To make it easier to understand, here are two examples, one from a regular cycle and another that results in pregnancy. Of course, this by itself isn’t totally reliable and other methods, such as Billings, should complement it.
Billings Method: It’s so simple that women of all ages can use it to conceive or avoid pregnancy. It’s based on cervical mucus, a secretion that comes out of the vagina throughout the cycle. Typically, its consistency is stretchy and has an egg white appearance. However, other women may also be fertile with watery (very runny, clear) mucus or soap-like mucus (slippery, white or clear). What’s important to notice in this method is: the more moist a woman is in the intimate area, the more fertile she is, and the stretchier the mucus, the better. We can say that mucus is the clearest sign that ovulation is about to happen, even if a woman finished her period just a few days ago.
Ovulation Test Method: This is a test like those sold in pharmacies for pregnancy or even through sellers who import well-known brands like OPK. Ovulation tests work the same way as pregnancy tests, but instead of detecting hCG (pregnancy hormone), they detect LH, which is what stimulates ovulation. It’s very effective and simple to use, and is recommended even for women with very regular cycles.
I can say and conclude that the three methods complement each other, and a woman trying to conceive who knows all of them can, indeed, get pregnant more easily. But as perfect and easy as it may seem, it isn’t always!
Common Problems
Some women trying to conceive may have more serious fertility problems and may try for years. For them, things often start with a marathon of medical appointments, undergoing all sorts of exams to detect (or rule out) issues preventing the couple from achieving pregnancy. But what are the most recurring problems that cause the most headaches?
As we saw earlier, women with polycystic ovaries are candidates for serious problems, both because they don’t know their ovulation periods or because of hormonal issues. In fact, hormones are one of the villains and can play tricks on women TTC. So, having your hormonal exams up to date is more than just basic, both for women with polycystic ovaries and for those with no history of hormonal problems. Always remember that the deficiency of just one hormone among the thousands present in our body can prevent pregnancy!
Prolactin (the hormone that helps produce breast milk), estrogen or even progesterone – any one of these simple hormones can sabotage a woman during her attempts to conceive by preventing ovulation. That’s why the gynecologist should, first and foremost, check the state of these hormones to rule out any related problems and begin looking for the real inhibitor of pregnancy.
I personally had terrible hormonal problems with some of them being out of control, not to mention my husband’s varicocele or my anovulation. They made me wait more than three years for a positive. They all gave me a headache to resolve, but eventually the positive arrived. So, I say from experience: keep your exams up to date! Are your hormones in check? Yes? Then it’s time for ultrasound scans.
Besides hormones, the uterus is the main actor in trying to have a baby. It must be clean and prepared for pregnancy to happen quickly and without major concerns. Any issues like fibroids or bicornuate or septate uterus (where the uterus is divided in half, but with different sizes) can be obstacles. However, even with these issues, it’s not impossible to naturally get pregnant. The importance of the ultrasound exam, just like hormonal exams, is really to discover any possible cause that might prevent the baby from reaching your arms.
Normally, when doctors suspect a more serious problem like tubal adhesions or endometriosis, they recommend exams such as:
- Hysterosalpingography
- Pelvic Ultrasound
- Resonance Imaging
- Blood Tests (Rh Factor, Sexually Transmitted Diseases, etc.)
And if there’s any problem, what then? The doctor following your case will guide and prescribe medication if necessary. But friend, if you don’t feel safe or don’t have 100% trust in your doctor, nothing stops you from seeking a second opinion from another professional. You can even look for several doctors until you find one you trust and feel comfortable with.
Also, remember that a child is made by a couple, right? A very relevant piece of advice is always to highlight the importance of exams for the man, husband or partner. I’ve seen many cases where a woman blames and punishes herself for years of unsuccessful tries, and the problem actually lay with her partner. Varicocele (inflammation of the veins in the testicle) and even a simple inflammation are typical problems that can be easily resolved. For these investigations regarding your partner, the urologist is the recommended specialist. But your gynecologist can also help during the investigation, providing referrals for the most routine exams like blood and urine tests, or even a semen analysis.
If you suspect your partner may have a problem, book, before anything else, an appointment with a urologist and then with a trustworthy gynecologist. The doctor should be the couple’s best friend in their journey to conceive. If any impediment is found, he will either monitor the situation or refer you to a specialist.




